
 RTI Act
RTI Act
Tooth demineralization and caries detection
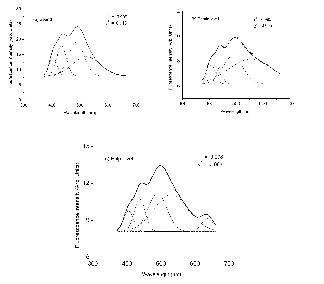
Fig. 1. The curve-fitted LIF spectra of sound, dentine level and pulp level caries from in vitro tooth samples with 337nm laser laser excitation.
For decades, dentists have relied on visual inspection, tactile examination with probe and X-rays to identify dental caries and early-stage cavitation sites. Among these, visual inspection is the favoured choice to diagnose dental caries because it is non-destructive as compared to mechanical methods such as probing, which can damage tooth structure and X-rays, which are ionizing and hazardous in nature. All of these methods have limitations affecting either their diagnostic ability or their practicality in a clinical setting. Once the caries cavity is detected by conventional techniques, tooth demineralization has usually progressed through approximately one-third to one-half of the enamel’s total thickness. Since X-rays only show good contrast when considerable mineral loss has already taken place, this technique allows detection only of already well-advanced caries. At this stage, the treatment option is drilling and filling with restorative material. Thus there is an emerging need for sensitive, clinically relevant non-invasive methods for early detection and quantification of caries lesions.

Fig. 2. Clinical trials with the LIFRS system at the Govt Dental College, Trivandrum with the inset showing the close-up
One of the significant aspects in dental caries diagnosis is that if early changes are not detected, lesion would continue to demineralize, which eventually leads to cavity formation. Once cavitation occurs, the lost tooth structure cannot be regenerated. It may be noted that tooth demineralization is difficult to diagnose in the early stages of development with the existing detection methods. Therefore, the main focus was to explore the potential of laser-induced fluorescence (LIF) and diffuse reflectance (DR) spectroscopic techniques to identify incipient changes in tooth enamel, which is crucial for decisions on treatment modalities in operative dentistry.
We have studied in detail the LIF and DR spectral features of caries tooth under different stages of caries formation both under in vitro and in vivo conditions jointly with the Chitra Dental Clinic and Govt Dental College, Trivandrum. In vitro studies using nitrogen laser excitation has shown that LIF spectral features identify the stage of caries and spectral analysis using curve-fitting technique improves the detection sensitivities (Fig. 1).
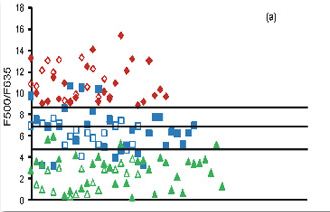
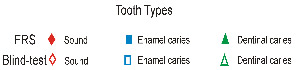
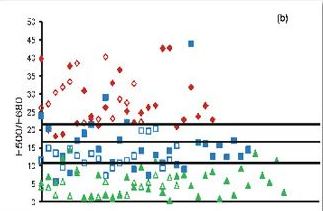
Fig. 3. Fluorescence ratio algorithm developed from 65 patients, diagnosed as incipient and advanced caries lesions, along with the 25 sites of sound teeth for a) F500/F635 and b) F500/F680 ratios. The solid symbols represent FRS ratios whereas the hollow symbols represent the blind test results from 40 patients.
In the clinical trials a diode laser emitting at 404 nm was used for excitation of fluorescence (Fig. 2). The LIF spectra of sound tooth showed a broad peak at 500 nm whereas two additional peaks were seen at 635 and 680 nm in caries tooth. In advanced caries 500 nm tooth broadens and shifts by 30 nm towards the red spectral region and the peaks at 635 and 680 become more intense. The results of this clinical study illustrate that information provided by non-invasive LIF spectroscopy has excellent potential to detect dental caries in its early stage. The fluorescence ratio (F500/F635 and F500/F680) diagnostic algorithms based on tissue autofluorescence were found to be sensitive and specific in discriminating different stages of tooth caries and in detecting early changes in tooth enamel that lead to caries formation (Fig. 3). Among the various ratios studied, F500/F635 ratio was found more suitable for detecting early tooth caries with 100% sensitivity and 97% specificity with PPV of 0.97 and NPV of 1.00. Our results confirm that the classification of tooth caries with 404 nm excitation allows precise visualization and quantification of both the dental hard tissues from the intrinsic green fluorescence as well as the red fluorescence of bacterial origin. Further studies are necessary to test the efficacy of LIF in detecting secondary caries.