
 RTI Act
RTI ActPeriodontitis is a multifactorial inflammatory disease involving both soft and hard tissues surrounding the teeth that leads to progressive destruction of the periodontal ligament and alveolar bone resulting in clinical features such as pocket formation, gingival recession, or mobility. It is an endemic infectious disease affecting the tissues surrounding the teeth, which results in significant debilitation for about half of the affected persons. Periodontal diseases begin as gingivitis and progress slowly towards periodontitis.
Gingivitis is the presence of gingival inflammation without the loss of connective tissue attachment, whereas periodontitis is the inflammation of the periodontium characterized by pathological detachment of collagen fibers from cementum with the junctional epithelium migrated apically. Inflammatory events associated with connective tissue attachment loss also lead to the resorption of coronal portions of tooth supporting the alveolar bone. Recent studies have revealed the influence of periodontitis on increased risk of vascular diseases, diabetes mellitus, lung diseases, and preterm delivery.
The gold standard for diagnosis of periodontitis is the clinical level of periodontal attachment. The parameters used in routine clinical practice to evaluate the status of periodontal disease are periodontal probing depth and bleeding on probing. Nevertheless, probe penetration is affected by the inflammatory status of periodontal tissue. The poor reliability and reproducibility associated with the measurement of clinical attachment level to monitor the progression of periodontal destruction and to evaluate the effect of periodontal treatment limit the practical value of periodontal probing, despite its popular use.
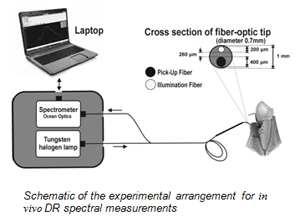 CESS has developed an optical spectroscopy technique based on diffuse reflectance of tissues for non-invasive detection of oral cavity cancer. A clinical study was carried out jointly with the Government Dental College, Thiruvananthpuram, to extend the applicability of this technique in the quantification and discrimination of periodontitis and gingivitis from healthy gingiva. DR spectral measurements were carried out with white-light illumination from 70 healthy sites in 30 healthy volunteers, and 63 gingivitis- and 58 periodontitis-infected sites in 60 patients. Clinical parameters such as probing pocket depth, clinical attachment level, and gingival index were recorded in patient population. Diagnostic accuracies for discrimination of gingivitis and periodontitis from healthy gingiva were determined by comparison of spectral signatures with clinical parameters. Divergence of average DR spectral intensity ratio between control and test groups was studied using analysis of variance. The mean DR spectrum on normalization at 620 nm showed marked differences between healthy tissue, gingivitis, and periodontitis. Hemoglobin concentration and apparent SO2 (oxygen saturation) were also calculated for healthy, gingivitis, and periodontitis sites. DR spectral intensities at 545 and 575 nm showed a decreasing trend with progression of disease. Among the various DR intensity ratios studied, the R620/R575 ratio provided a sensitivity of 90% and specificity of 94% for discrimination of healthy tissues from gingivitis and a sensitivity of 91% and specificity of 100% for discrimination of gingivitis from periodontitis.
CESS has developed an optical spectroscopy technique based on diffuse reflectance of tissues for non-invasive detection of oral cavity cancer. A clinical study was carried out jointly with the Government Dental College, Thiruvananthpuram, to extend the applicability of this technique in the quantification and discrimination of periodontitis and gingivitis from healthy gingiva. DR spectral measurements were carried out with white-light illumination from 70 healthy sites in 30 healthy volunteers, and 63 gingivitis- and 58 periodontitis-infected sites in 60 patients. Clinical parameters such as probing pocket depth, clinical attachment level, and gingival index were recorded in patient population. Diagnostic accuracies for discrimination of gingivitis and periodontitis from healthy gingiva were determined by comparison of spectral signatures with clinical parameters. Divergence of average DR spectral intensity ratio between control and test groups was studied using analysis of variance. The mean DR spectrum on normalization at 620 nm showed marked differences between healthy tissue, gingivitis, and periodontitis. Hemoglobin concentration and apparent SO2 (oxygen saturation) were also calculated for healthy, gingivitis, and periodontitis sites. DR spectral intensities at 545 and 575 nm showed a decreasing trend with progression of disease. Among the various DR intensity ratios studied, the R620/R575 ratio provided a sensitivity of 90% and specificity of 94% for discrimination of healthy tissues from gingivitis and a sensitivity of 91% and specificity of 100% for discrimination of gingivitis from periodontitis.
The results of this study are published in the March 2012 issue of the Journal of Biomedical Optics.
